The Haller Method produces Clinical Outcome Speeds that, without the visuals and video evidence would be unbelievable in this medium. My clients and my students see it every day. These effects are gained by implementing the principles from Foundations for Clinical Neuroplasticity also known as the Haller Method .
In the process of developing theories and approaches, every person need giants on whose shoulders they can stand. Two of my inspirations are Donald Hebb and Michael Merzenich.

Hebb established that: “What fires together, wires together”
I think it may be possible to summarise some of Michael Merzenich’s work as:
“What is ignored is pruned.”
These 2 principles underpin my interventions, my practice and my teaching.
And they apply when looking at human development, which is set up to happen in a specific sequence with growth and pruning cycles. If this sequence is disrupted at any point there are gaps in connectivity. These gaps can be interpreted as missing neural connections that show up in muscular contraction patterns.

Everything we ever do is done through muscular contractions.
No muscular contraction = death
The fewer the connectivity gaps – the more sophisticated the muscular contractions possible, making for a huge, huge diversity of combinations and patterns of contractions available.
This results in more available choice of response to any given stimulus – a state that is often experienced as maturity.
So, the Clinical Question is:
How does a clinician identify and then fill the gaps?
I use an aggregated, 5 factor approach to identify and fill neural gaps – in a sequence that causes predictable neural cascades, which in turn increases the rate of change. The application of this is what I teach in my classes and what I use in my clinic.

As an Occupational Therapist, it is my job to find the glitch point in my client’s dysfunction that is blocking their improvement. This is point of task analysis, the kingpin of Occupational Therapy.
To bring about change in function I usually have to bring about a different set of muscular contractions and have found that if you cannot find a targetted muscle, you cannot move it.
If you cannot move it, you cannot do things differently.
This is the foundational thinking for what I do. It led to the formulation & use of the 5 factor approach that both identifies the gaps & directs the remediation
When working with children, where we are starting from the beginning building the brain and its connections, clinicians are seeing very significant speed of change in language, awareness and function when interventions are targeted and in developmental sequence.
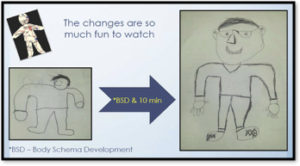
This drawing is an example of the changes that can occur within 10 minutes in a child’s perceived body schema after doing connectivity exercises – which are the center thought of the approach.
Addressing trauma and stress are some of the most crucial interventions we participate in, as very little neuroplastic change happens when perceived safety is challenged. The combination of using attunement and kinesiology principles allows a therapist to cut to the heart of issues.
Understanding how stress profiles manifest in our relational styles and can influence our perceived safety opens doors to establishing an internal locus of control.
Considering the impact of nutrition or toxicity on perceived safety has changed many lives and there are more and more studies showing the validity of including GUT health in all rehab approaches.
The last, but not least important engagement in growing neural connections deals with the actual nerves and muscles. The previous 4 are set-up engagements to allow for optimal neural growth – which will allow for greatest range of choice of response to any given stimuli. In other words, the most maturity. The easiest access paths for facilitating this particular growth is using primitive reflexes as they are easy to identify, are fundamental to all movement and when inappropriately active have vastly disruptive effects on all brain function. This includes emotional and executive function. Ensuring their correct expression allows for jumps in function that have been thought to be impossible.
Through-out our treatments over a 5 year period (2013-2017) a definite pattern emerged that is documented in the pilot study I wrote up and which was selected to be published by the Journal of Functional Neurology, Rehabilitation and Ergonomics. As a result of the Haller Method of addressing all 5 factors, not only were impairment decreases evident but rates of in-session progress were much better than expected. That means that the actual number of required sessions to reach initial goals was drastically reduced.
I still find this to be the case and as I have explored this medium, it has become even more predictable.
This affects the cost-benefit ratio for clients and all payor sources – which in an increasing factor in therapy. If the clinic is private pay – like mine is – this is huge.
Two case studies:
The first is Micha – she is 9 years old. When she came to me, she was having enough trouble with academic tasks such as reading and math that she required tutors, was on a specialized intervention program and had started exhibiting defiant and combative behaviours at home. I saw her 1x a week for 12 weeks. By the end of those sessions she was reading voluntarily, was pleasant and doing quite well at school. After the second 12 week series she was acing Spanish, managing spelling on her own and in general her competency, self esteem and demeanor have risen in leaps and bounds

The Haller method of clinical interventions does not only work with Children. Adults benefit too
Arlene is a stroke victim. Strokes are not that different from other induced central nervous system dysfunction including mental health. Adult stroke does however often have the component of an underlying, already developed neural structure which just needs reconnecting of the appropriate parts.

After Arlene’s stroke and discharge from hospital, about 2 years ago, she was treated using the 5 factors of the Haller method. She was able to reach functional status within 3 months – despite her doctor’s prognosis that recovery would not be possible.
Arlene had the added support of her daughter and her community in participating and performing the Home Exercise Program.
An extremely condensed video of her progress in my first 40 minute session is available by clicking here. At the end, there is a clip of the 4th and final session I had with her and some pictures of her regained functional tasks.
If you watch the video, notice the following changes:
Firstly – the clarity of her speech as the first session progresses.
Secondly – her facial animation and awareness
At the end notice her balance and her emotional engagement
This is Arlene’s Rapid Road to Recovery.
It is not that she recovered is remarkable – it is that it happened so fast.
This is the point of the Haller Method. It really is a holistic way of looking at creating developmental and recovery options for those who wish to explore them. It takes the person, as a whole, many faceted being, into account and factors in the inter-dependency of human systems to create faster outcomes.
The Haller Method is a therapeutic approach. It is not meant to be applied in arenas that do not allow touch, have rigid protocol driven interventions or do not allow for whole person responses. It is best suited to Occupational Therapists, but can be applied by other disciplines open to embracing the complexity of humans, their processing systems and their need for safety before growth.